70 year old male with fever and weakness
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problems with collective current based inputs.
70 year old male with
1)fever since 15 days
2)generalised weakness and body pains in bilateral lower limbs since 10 days
HOPI
Pt was apparently asymptomatic 15 days back then had fever which high grade more during night time associated with chills and rigors it is intermittent not associated with cold , cough, vomitings , loose motions, abdominal pain, burning micturition , no h/o rash, hematuria, bleeding from gums
For which he was taken to local rmp and got treated for the same and diagnosed typhoid fever and reports from outside showing platelets of 85,000
Then he had generalised body weakness and pains in bilateral lower limbs and lower back ache since 3days. Pt is unable to walk or stand without support since 3 days
DAILY ROUTINE
He wakes up at morning 6 does his daily routine and takes rice at 8:00-9:00am goes to work ( farmer) and takes food at 1:00pm returns home at 5:00 pm and takes dinner at 8:00pm qnd goes to sleep
PAST HISTORY
not a known case of HTN ,DM ,ASTHMA, EPILEPSY , TB,CAD
FAMILY HISTORY
Not significant
PERSONAL HISTORY
Diet - mixed
Appetite- decreased
Bowel and bladder movements- regular
sleep- inadequate
Addictions- takes beedis and chutta daily 4 to 5 since 30years
consumes alcohol occasionally since 30 years
GENERAL EXAMINATION
pt is conscious coherent notcooperative well oriented to time place person
pallor-absent
icterus- absent
clubbing- absent
cyanosis- absent
edema - absent
lymphadenopathy- absent
VITALS( at admission)
BP - 130/90mm hg
PR- 76bpm
RR- 26cpm
TEMP- 98.6°F

SYSTEMIC EXAMINATION
CVS - S1, S2 heard
RS - BAE present
PA - soft , non tender
CNS-


VIRAL PYREXIA ? CEREBELLAR ATAXIA
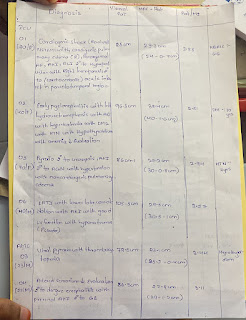
INVESTIGAGIONS
outside investigations


4/09/2022















2) INJ CEFTRIAXONE 1gm IV BD
3)INJ NEOMOL 1gm IV / SOS( if temp >101°F)
4) INJ ZOFER 4mg sos
5) TAB PCM 650 mg PO TID
6) TAB PAN 40 mg IV SOS
7) INJ OPTINEURON 1amp in 100 ml NS IV OD
8) TAB MVT PO OD
9) TEMP MONITORING 2nd hely
10) BP, PR monitoring 4th hrly
11) GRBS monitoring 6th hrly
3)INJ NEOMOL 1gm IV / SOS( if temp >101°F)
4) INJ ZOFER 4mg sos
5) TAB PCM 650 mg PO TID
6) TAB PAN 40 mg IV SOS
7) INJ OPTINEURON 1amp in 100 ml NS IV OD
8) TAB MVT PO OD
10) BP, PR monitoring 4th hrly
11) GRBS monitoring 6th hrly
2) INJ CEFTRIAXONE 1gm IV BD
3)INJ NEOMOL 1gm IV / SOS( if temp >101°F)
4) INJ ZOFER 4mg sos
5) TAB PCM 650 mg PO TID
6) TAB PAN 40 mg IV SOS
7) INJ OPTINEURON 1amp in 100 ml NS IV OD
8) TAB MVT PO OD
9) TAB HIFENAC PO/ BD
10) TAB NEUROKIND LC HS
11)TEMP MONITORING 2nd hrly
12) BP, PR monitoring 4th hrly
13) GRBS monitoring 6th hrly
2) Tab CEFIXIME 200mg PO/BD
3)TAB PCM 650 mg PO/ SOS
4)TAB PAN 40 mg Po/OD
5) TAB MVT PO/ OD
6)TAB HIFENAC PO/BD
7) TAB NEUROKIND LC H/S


Comments
Post a Comment