56 year old male with fever and loss of consciousness
This is online E-blog, to discuss our patient de-identified health data shared after taking her guardian's signed informed consent.
Here we discuss our individual patient problems through series of inputs from available global online community of experts with an aim to solve the patients clinical problem with current best evidence based input.
This E-blog also reflects my patient's centred online learning portfolio.
I have been given this case to solve in an attempt to understand the topic of "Patient Clinical Data Analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan.
Following is the view of
CASE
56 year old male patient came to opd on 28/08/2021 with chief complaints of
Fever since 3 days
loss of consciousness for 5 mins on 28th morning
HISTORY OF PRESENTING ILLNESS
• Patient developed fever which was insidious in onset and continuous type no diurnal variations seen, low grade fever,he had cold and dry cough,associated with chills and rigors not associated with body aches, vomitings, abdomen pain, loose motions
•On 28th of august when patient woke up for urination at 5 am he had giddiness, shivering and up rolling of eyes , no involuntary movements , no tonic movements then they went to rmp and referred here
• Pt on presentation - had SBP - 70 mm hg ( Hypotension)
• He experiencing incresed frequency on urination about 20 times per day , there is no urgency , difficulty in passing urine, no pain while passing urine , no hematuria
• Trombhophlebitis on 30thof august
• 2 / 09/2021- there is decreased in the frequency of urination than before
PAST HISTORY
•10 years back pt had developed sudden weakness ( unable to hold any thing)of left upper limb and lower limb which was sudden in onset for which he was hospitalized for 1 week following which there was slight improvement
•4 years back he developed weakness in right upper limb and lower limb and for which hospitalized and slight improvement is seen but not as much as left limbs
•10 days back at field while passing urine he had giddiness and fell down and had injury over right knee and face and then had taken injection from Rmp
•Not a known case of diabetes ,hypertension ,asthma, epilepsy,
• CVA - 10 years ago
PERSONAL HISTORY
•Diet:- mixed
•Appetite:- normal
• Bowel and bladder movements :- increased frequency of urination since 29th and , not passed stool since 2 days •Habits:- chronic alocholic 10 yrs back then stopped consuming then resumed 4 years ago and then stopped consumed then after
FAMILY HISTORY
not significant
GENERAL EXAMINATION
Patient was conscious cohorent cooperative well oriented to time , place , person, moderately built and moderately nourished
Pallor - absent
Icterus- absent
Cyanosis- absent
Clubbing- absent
Lymphadenopathy- absent
Edema- absent
VITALS
PR- 67 bpm
RR- 25cpm
BP-90/60mm hg
Spo2- 98%
GRBS-151 mg%


SYSTEMIC EXAMINATION
•CVS- s1 ,s2 heard no murmurs
• Respiratory system- normal vesicular breath sounds heard
• Abdomen- no tenderness seen, no palpable mass seen, not distended
• CNS-
▪ sensory examination,- touch, pain , vibration present
▪ No muscle wasting seen
▪ Hypertonia of lower limbs and clasp knife spasticity in left upper limb
▪ Power of muscle
• upper limb
rt. lt
Biceps. 5/5. 5/5
Triceps. 5/5. 4/5
Opponens pollices
5/5. 4/5
• lower limb
Extensors of knee
4-/5. 4-/5 Flexors of knee
4-/5. 4-/5
Exetnsors of hip
4-/5. 4-/5
External hallucis longus
4-/5. 4-/5
▪Reflexes
• Deep tendon reflexes
Knee jerk. +3. +3
Ankle reflex +3 +3
Biceps. +3. +3
Triceps. +3 +3
Supinator. +3. +3
• Superficial reflexes
Babinskis sign - seen on both sides
Abdominal reflex - present
▪Coordination
• Finger nose test- no incoordinatino is seen
• knee heel test- unable tooperform on rigth ides
• Romberg sign- negative
▪Antalgic gait
▪ Cranial nerve examination
•CN -1- normal
•CN- 2 - patient cannot see clearly both near and far
•CN-3,4,6- movement of eye balls normal in all directions, in both the eyes ,
Light reflex and consensual light reflex absent ,
Accommodative reflex - constriction of pupil is not seen, adduction. of eyes seen
ANISOCORIA - seen
, Dilated pupil- lt eye


















• CN- 5- both sensory and motor components are normal
• CN-7 - normal
• CN-8- rinnes test - positive on both sides
webber - no latearlisation seen
• CN- 9 - normal
• CN-10- normal
• CN-11- normal
• CN-12- normal
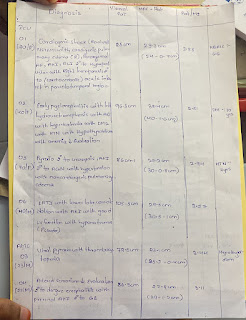
INVESTIGATIONS

28/08/2021

31/ 08/2021

31/08/2021

28/08/2021

30/08/2021

30/08/2021

30/08/2021

28/08/2021

28/08/2021


28/08/2021

ECG






DIAGNOSIS- VIRAL PYREXIA WITH PREVIOUS HISTORY OF QUADRIPARESIS
TREATMENT
29/ 08/2021
IVF - NS , RL@ 100ml/hr
INJ- pantop 40 mg IV/OD
INJ- noradrenaline@4ml/hr
BP, PR,RR monitoring
Temp 4th hourly
Sritct I/O charting
30/08/2021
IVF - NS , RL@ 100ml/hr
INJ- pantop 40 mg IV/OD
BP, PR,RR monitoring
Temp 4th hourly
Sritct I/O charting
Tab- dolo650 mg
InJ - Neomol 100ml/ IV / stat
31/08/2021
IVF - NS , RL@ 100ml/hr
INJ- pantop 40 mg IV/OD
Tab- dolo650 mg
InJ - Neomol 100ml/ IV / stat
BP, PR,RR monitoring
1/09/2021
IVF - NS , RL@ 100ml/hr
INJ- pantop 40 mg IV/OD
Tab- dolo650 mg( check temp before giving dolo
BP, PR,RR monitoring
Syp- ascoril
InJ - Neomol 100ml/ IV / stat( if temp increases)
Thrombophube ontmient


{kind=link}
Comments
Post a Comment