1) Covid 19 with co morbidity (Pulmonology/Rheumatology)Case -1
https://nikhilasampathkumar.blogspot.com/2021/05/covid-pneumonia-in-pre-existing-case-of.html
1) How does the pre-existing ILD determine the prognosis of this patient?
•Patients with pre existing ILD have poor prognosis
•Patients with preexisting ILD may be at high risk for severe COVID-19 disease due to impaired lung function, propensity to develop acute exacerbation of pulmonary fibrosis or immunomodulatory medications that may interact with viral clearance or pathogenesis,
•Mortality due to COVID-19 was higher in patients with preexisting fibrotic idiopathic interstitial lung disease compared with other interstitial lung diseases, researchers reported in a new study.
https://www.healio.com/news/pulmonology/20201217/mortality-due-to-covid19-elevated-in-patients-with-preexisting-ild
Interstitial lung disease (ILD) is characterized by injury to the alveolar epithelium and abnormal wound healing (8). Patients with ILD have diminished pulmonary reserve and impaired gas exchange. Viral infections can trigger acute exacerbations, which are associated with poor outcomes (9). Many patients with ILD are on immunosuppressive medications. It stands to reason that patients with ILD would have an increased rate of complications and death from COVID-19.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7737597/
2) Given the history of autoimmune disease in the patient, how does the administration of steroids for COVID affect her RA and hypothyroidism?
3) Would this patient have an increased risk for post covid autoimmune response compared to patients without a history of autoimmune disease?
YES,The development of autoimmune conditions subsequent to COVID-19 infection could be related to both factors: transient immunosuppression of innate and acquired immunity leading to a loss of self-tolerance to self-antigens, and a form of inappropriate immune reconstitution in individuals with predisposing conditions of autoimmunity
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7556280/
4) Why was she prescribed clexane (enoxaparin)?
▪Patients with COVID-19 are at high risk of developing a venous thromboembolism (VTE) and it is essential that effective thromboprophylaxis with parenteral drugs (LMWH, UFH) is considered for all patients admitted to hospital especially in case of severe pneumonia
▪IL-6 levels are highly elevated in patients with severe disease,Enoxaparin is said to relieve and prevent inflammation produced by IL-6 by inactivating it by binding it with its non-anticoagulant fraction, especially in pulmonary epithelial cells.
https://clinicaltrials.gov/ct2/show/NCT04646655
Case 2
2) Covid 19 with Diabetes
https://nehapradeep99.blogspot.com/2021/05/a-50-year-old-female-with-viral.html
1) Since patient didn't show any previous characteristic diabetes signs, did the Covid-19 infection aggravate any underlying condition and cause the indolent diabetes to express itself? If so what could be the biochemical pathways that make it plausible?
▪There is a bidirectional relationship between Covid-19 and diabetes
▪On the one hand, diabetes is associated with an increased risk of severe Covid-19. On the other hand, new-onset diabetes and severe metabolic complications of preexisting diabetes, including diabetic ketoacidosis and hyperosmolarity for which exceptionally high doses of insulin are warranted, have been observed in patients with Covid-19.1
▪Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the virus that causes Covid-19, binds to angiotensin-converting enzyme 2 (ACE2) receptors, which are expressed in key metabolic organs and tissues, including pancreatic beta cells, adipose tissue, the small intestine, and the kidneys.4 Thus, it is plausible that SARS-CoV-2 may cause pleiotropic alterations of glucose metabolism that could complicate the pathophysiology of preexisting diabetes or lead to new mechanisms of disease.
https://www.nejm.org/doi/full/10.1056/nejmc2018688
2) Did the patient's diabetic condition influence the progression of her pneumonia?
▪ Yes, with DM or hypergycemia in patients leads to an increase in COVID-19 severity. Also, poor glycaemic control predicts an increased need for medications and hospitalizations, and increased mortality.
▪In monocytes: elevated glucose levels increase SARS-CoV-2 replication, and glycolysis sustains SARS-CoV-2 replication via the production of mitochondrial reactive oxygen species and activation of hypoxia-inducible factor 1α. Therefore, hyperglycaemia supports viral proliferation
▪There may be increased chance of morarality in diabetic patients.
https://care.diabetesjournals.org/content/30/9/2251
Pathophysiology of SARS-CoV-2 in lung of diabetes3) What is the role of D Dimer in the monitoring of covid? Does it change management or would be considered overtesting?
▪D-dimer is a fibrin degradation product that is often used to measure and assess clot formation.
▪As we all know, the deadly virus can form a colony in the lungs and turn more dangerous than we can even think of. Rare symptoms like blood clotting are also being seen and this is the major reason why the D-dimer test is undeniably important
▪D-dimer test appropriately shows the presence of blood clots in the patient's body, even in lungs, who are having severe forms of Covid-19. In such conditions, the patient may face shortness of breath and difficulty in breathing. A D-dimer test is the ultimate solution in such cases
▪D- Dimer does change the management, as D-Dimer levels above 2000ng/dl were found to have a direct link with increasing severity of COVID-19 [7]. Moreover, D- dimer levels would be helpful in fast diagnosis and prevention of thrombotic complications.
(COVID-19 SEVERE)
1. Why was this patient given noradrenaline?
2. What is the reason behind testing for LDH levels in this patient?
▪The lactatedehydrogenase (LDH) test looks for signs of damage to the body's tissues. LDH is an enzyme found in almost every cell of your body, including your blood, muscles, brain, kidneys, and pancreas. The enzyme turns sugar into energy. The LDH test measures the amount of LDH in your blood or other body fluid
▪In this patient, an increase in LDH levels would denote inflammation, and a high increase would denote Multi-Organ Failure.
3. What is the reason for switching from BiPAP to mechanical ventilation with intubation in this patient? What advantages did it provide?
Although BiPaP is a positive pressure system, unlike tracheal intubation, it does not send the air to the trachea and depends on the patient's ability to respire. In this patient, as SpO2 levels were dropping to 30% despite BiPAP, a more invasive method was required to push the air directly into the lungs- hence intubation was preferred.
Case-4
1. Is the elevated ESR due to covid related inflammation?
▪An erythrocyte sedimentation rate (ESR) is a type of blood test that measures how quickly erythrocytes (red blood cells) settle at the bottom of a test tube that contains a blood sample.
▪Normally, red blood cells settle relatively slowly.
▪A faster-than-normal rate may indicate inflammation in the body. Inflammation is part of your immune response system. It can be a reaction to an infection or injury
▪In this condition patient has covid infection so it may be covid related
2. What was the reason for this patient's admission with mild covid? What are the challenges in home isolation and harms of hospitalization?
▪Hospitalisation was due to Grade 3 Shortness of Breath (SOB), and long duration of COVID-19 infection.
▪Challenges of home isolation-
•Physical challenges- Many patients may find it hard to cut themselves from the outside world and confine themselves to a room for long periods of time
Emotional challenges- Sitting in a small room all day leads to stress, anxiety and even depression, with an increase in mental health issues being reported during the pandemic
•Social challenges- Members of society who cannot care for themselves on their own (eg, patients with disability, geriatric patients etc) are at a major loss
Economic challenges- Some patients, such as daily wage labourers, cannot afford to home isolate as they need to earn on a daily basis to keep their family going
▪Harms of hospitalisation-
•Infection- Members visiting may get COVID from exposure to the hospital ward alone
•Cost- PAtient may not be able to bear the brunt of high costs
•Overtesting- Hospitals may ask the patients to stay overnight despite the conditions being mild, based on preliminary test results
•Economic- Working patients may have to take a leave of absence, hence affecting both their work and decreasing their salary, on top of spending money on hospitalisation
1) What was the reason for coma in this patient?
▪The reason for coma is due to severe hypoxia, as his SpO2 levels were 20% when he was admitted.
▪Along with this, hypokalemia leads to respiratory muscle paralysis, which may have aggravated his dyspnoea.
2) What were the competency gaps in hospital 1 Team to manage this intubated comatose patient that he had to be sent to hospital 2? Why and how did hospital 2 make a diagnosis of hypokalemic periodic paralysis? Was the coma related?
▪The main competency gap was in the lack of testing for serum electrolytes, as the hypokalemia had caused weakness and fatigue in this patient.
▪Hospital 2 make a diagnosis of hypokalemic periodic paralysis based on the fact that the patient had generalised weakness before becoming comatose, along with tingling and symptoms of paralysis. On testing serum electrolytes, his potassium levels were found to be 2.3 mEq/L (normal-3.5-5)
▪The coma was most probably related, as hypokalemia can cause respiratory muscle paralysis, leading to aggravation of hypoxia, hence causing unconsciousness in the patient.
3) How may covid 19 cause coma?
▪Yes, as the brain is extremely sensitive to oxygen, oxygen deprivation due to COVID-19 can lead to a comatose state.
▪This patient had very low SpO2 levels (20%), which may have caused the coma.
Case-6
COVID-19 WITH ALTERED SENSORIUM
1. What was the cause of his altered sensorium?
Altered sensorium due to hypoxia, leading to hypercapnic encephalopthy and altered sensorium
Increased urea levels leading to uraemic encephalopathy, which causes altered sensorium
2. what is the cause of death in this patient?
The cause of death in this patients was due to complications of COVID-19, most probably Acute Kidney Failure (AKI), as denoted by increased urea and creatinine, and hypoproteinemia. Hypoxia and inflammatory response due to COVID-19 may have triggered the process.
Case-7
1. What is the grade of pneumonia in her?
In this patient CT severity score is 12/25,
so patient pneumonia is moderate
2. What is the ideal day to start steroids in a patient with mild elevated serum markers for COVID ?
Dxamethasoe can be given for mild disease before the onset of cytokine strom,it inhibits the macrophage mediate inflammation
3.What all could be the factors that led to psychosis in her ?
•Sensory deprivation
•Sleep deprivation
•Stress
•Continuous light levels
•Continuous monitoring
•Lack of orientation
•Pain
•Drug reactions
•Infections
•Metabolic disorders
•Dehydration
4.In what ways shall the two drugs prescribed to her for psychosis help ?
▪Piracetam is a nootropic drug that improves one or more aspects of mental functions, predominantly cognitive functions such as working memory, motivation and attention
•It improves the function of the neurotransmitter acetylcholine via muscarinic cholinergic (ACh) receptors, which are implicated in memory processes. Furthermore, piracetam may have an effect on NMDA glutamate receptors, which are involved with learning and memory processes
▪Risperidone is a medication that works in the brain to treat schizophrenia. It is also known as a second generation antipsychotic (SGA) or atypical antipsychotic. Risperidone rebalances dopamine and serotonin to improve thinking, mood, and behavior.
5. What all are the other means to manage such a case of psychosis?
•The management of ICU psychosis primarily depends on the cause. If it is sleep deprivation then the patient should be provided a peaceful place to take rest.
•If it is due to underlying conditions like heart failure and dehydration then these should first be corrected.
•Haloperidol is a medication commonly used to manage ICU psychosis. Other common anti-psychotics can also be used.
6. What all should the patient and their attendants be careful about ( w.r.t. COVID) after the patient is discharged ?
The patient is supposed to self isolate after they are discharged for another 7 days after discharge. If possible oxygen levels are to be monitored as well for the next 7 days. The patients and the patient's attenders should be on the look out for danger symptoms such as trouble breathing, chest pain, bluish discolouration of lips, confusion or inability to wake up.
7.What are the chances that this patient may go into long covid given that her "D Dimer" didn't come down during discharge?
A Long COVID is the persistence of symptoms such as cough, breathlessnes, headaches and chest pain weeks to months after discharge. People suffering from long COVID usually have elevated biomarkers such as elevated d dimer and CRP. As this patient has elevated d dimer levels at discharge there is a good chance that she could suffer from long covid
Case-81.Can psoriasis be a risk factor for severe form of COVID?
•At present, it is unclear how COVID-19 may affect those with psoriasis, which is an immune-mediated condition. This mean the condition occurs as a result of abnormal immune system activity
•Some treatments for psoriasis, which are immunosuppressive medications, may increase the risk of a COVID-19, or of severe illness due to the virus. However, the effects are .
•But the patient had psoriasis treatment 8
years back it might not be a. risk factor
2.Can the increased use of immunomodulatory therapies cause further complications in the survivors?
Immunomodulatory drugs more likely to play a role in cytokines strom and macrophage activation inpatients at risk of acquiring severe inflammation and death
By acting on immune system,all these drugs
may increase risk of infection
3. Is mechanical ventilation a risk factor for worsened fibroproliferative response in COVID survivors?
•Recent evidence demonstrate that mechanical ventilation particularly where significant out stretch ,occurs may drive the pathogenesis of fibrosis in a patients with ARDS
•Application of mechanical ventilation in in acute lung injury or application of stress in vitro in lung epithelial cells may induce the development of lung Fibrosis through fibroproliferative mechanism

case-9
Case-9
1. What is the type of DM the patient has developed ?(is it the incidental finding of type 2 DM or virus induced type 1DM)?
•Incedental type 2 DM can be differentiated from de novo covid induced type 1 DM with the help of the Hbc1 levels.
•As HbAc1 levels are indicators of long term blood sugar levels they are likely to be raised in pre existing DM that was incidentally discovered. But in case ofthe diabetes being de novo in nature then the HbAc1 levels are unlikely to be raised. As the patients HbAc1 levels are not raised we can not at this point determine if the patient has incedental discovered type 2 DM or Covid induced de novo DM.
2. Could it be steroid induced Diabetes in this patient?
•Dexamethasone is generally safe. It presents a favourable benefit-risk profile, particularly in patients with severe forms of pneumonia, while the benefit is less prominent in patients with non-severe pneumonia. As the treatment is short, even at high doses, corticosteroids are not associated with serious side effects. Potentially higher blood glucose levels (hyperglycaemia) are temporary.
Case -10
1. What are the known factors driving early recovery in covid?
•Younger age group
•Shorter duration of fever
•No past illness
•PaO2/FiO2 levels
•No perexisting lung pathologies
Case-11
1. How is the diabetes related to the prognosis of COVID patients? What are the factors precipitating diabetes in a patient developing both covid as well as Diabetes for the first time?
People suffering from diabetes are like to experience more severe symptoms of the disease than the ones who are not diabetic
2. Why couldn't the treating team start her on oral hypoglycemics earlier?
Aim is to reduce blood glucose levels as earlyr as possible,so As the insulin is faster acting as compared to oral hypoglycemics, so started on it
Case-12
1.What are the potential bio clinical markers in this patient that may have predicted the prolonged course of her illness?
•Serum LDH: 571U/L (Normal range=140-280U/L
•ALP : 342 U/L (Normal range=44-147U/L)
•SpO2: 82% at RA (Normal range= >96%)
•HR: 124bpm (Normal range=60-100bpm)
Classically, the bio clinical markers that are predictive of a Covid-19 patient's outcome are
•C reactive protein [>57.9mg/dL]
•D-Dimer [>1mcg/ml associated with poorer prognosis]
•Serum LDH [>248U/L]
•IL-6 [2.9 times higher in severe disease compared to mild disease]
•SGPT [Isolated rise in SGPT >3 times the normal value]
•ESR [high sustained level after recovery from infection]
•Albumin
•Platelet count
•Neutrophil count
•NLR: [>5.5]
•Urea
•Creatinine
•High sensitivity Troponin
•The patient in question has elevated levels of serum LDH and ALP. Her CRP and D-Dimer levels are not high enough to be considered as a bad prognostic factor.
Case-13
1) What are the consequences of uncontrolled hyperglycemia in covid patients?
•People with diabetes are more likely to have serious complications from COVID-19. In general, people with diabetes are more likely to have more severe symptoms and complications when infected with any virus.
•Your risk of getting very sick from COVID-19 is likely to be lower if your diabetes is well-managed. Having heart disease or other complications in addition to diabetes could worsen the chance of getting seriously ill from COVID-19, like other viral infections, because more than one condition makes it harder for your body to fight the infection.
•Viral infections can also increase inflammation, or internal swelling, in people with diabetes. This can also be caused by above-target blood sugars, and that inflammation could contribute to more severe complications.
•Control of blood sugar can also decrease the chances of a cytokine storm during the second phase of the infection.
https://www.diabetes.org/coronavirus-covid-19/how-coronavirus-impacts-people-with-diabetes#:~:text=A%3A%20People%20with%20diabetes%20are,your%20diabetes%20is%20well%2Dmanaged.

2) Does the significant rise in LDH suggests multiple organ failure?
•Severe infections may cause cytokine-mediated tissue damage and LDH release Since LDH is present in lung tissue (isozyme 3), patients with severe COVID-19 infections can be expected to release greater amounts of LDH in the circulation, as a severe form of interstitial pneumonia, often evolving into acute respiratory distress syndrome, is the hallmark of the disease.
•Elevated LDH values were associated with 6-fold increased odds of severe COVID-19 disease. More importantly, elevated LDH was associated with a >16-fold increase in odds of mortality.
•Elevated LDH levels seem to reflect that the multiple organ injury and failure may play a more prominent role in this pathology in influencing the clinical outcomes in patients with COVID-19.
3) What is the cause of death in this case?
•This patient was diagnosed with uncontrolled hyperglycemia with severe covid pneumonia.
•LFT shows elevated AST, ALT, and ALP with a gross increase in bilirubin titer.
•The D-Dimer is elevated (560ng/ml) and the LDH is 835U/L both of which are indicators of a poor prognosis.
•The most likely cause of death in this patient seems to be ARDS.
•The immediate cause of death: Most probably cardio-pulmonary arrest
•Antecedent cause: Severe covid-19 pneumonia.
Case-14
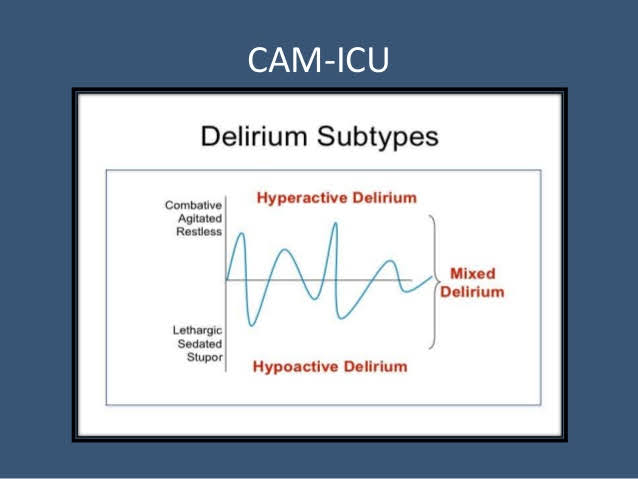
1)Which subtype of ICU psychosis did the patient land into according to his symptoms?
•ICU psychosis: A disorder in which patients in an intensive care unit (ICU) or a similar hospital setting may experience anxiety, become paranoid, hear voices, see things that are not there, become severely disoriented in time and place, become very agitated, even violent, etc.
•Three subtypes have been recognized: hyperactive, hypoactive, and mixed.
• Patient might be having Hyperactive delirium: Manifests as agitation, restlessness, refusal to cooperate with caregivers, unprovoked mood changes, hallucinations
2)What are the risk factors in the patient that has driven this case more towards ICU psychosis?
•Hypertension
•History of cerebrovascular accident (makes him more prone to a new one)
•Steroid use
•Sedative use (Gabapentin)
•COPD
3)The patient is sleep-deprived during his hospital stay. Which do you think might be the most probable condition?
A) Sleep deprivation causing ICU psychosis
B) ICU psychosis causing sleep deprivation
ICU psychosis causing sleep deprivation is more likely in this patient
4) What are the drivers toward current persistent hypoxia and long covid in this patient?
Elevated bio clinical markers like D-Dimer, LDH, Neutrophils, WBCs(absolute), IL-6, and CRP all contribute to persistent hypoxia and worsen the prognosis. In addition to this, ICU psychosis adds to the prolonged hospital stay.
Case-15
1. As the patient is a non-diabetic, can the use of steroids cause a transient rise in blood glucose?
Dexamethasone is generally safe. It presents a favourable benefit-risk profile, particularly in patients with severe forms of pneumonia, while the benefit is less prominent in patients with non-severe pneumonia. As the treatment is short, even at high doses, corticosteroids are not associated with serious side effects. Potentially higher blood glucose levels (hyperglycaemia) are temporary.
2. If yes, can this transient rise lead to long-term complications of New-onset diabetes mellitus?
In this context, there is accumulating evidence that hyperglycaemia at admission, both in DM subjects and in those with secondary hyperglycaemia, indicates a poor prognosis .
Importantly, newly diagnosed DM is linked to increased mortality, as compared with known DM and normal glucose levels in patients with COVID-19
3. How can this adversely affect the prognosis of the patient?
Hyperglycemia in general is indicative of a poorer prognosis in a patient compared to covid patients with normal blood glucose levels.
4. How can this transient hyperglycemia be treated to avoid complications and a bad prognosis?
Oral hypoglycemics (such as sulfonylureas) are efficient at controlling blood glucose levels in non-diabetics who develop steroid-induced hyperglycemia. Most cases revert to normoglycemia after discontinuation of steroids.
5. What is thrombophlebitis fever?
Fever in response to thrombophlebitis that is caused due to release of inflammatory mediators
6. Should the infusion be stopped in order to control the infusion thrombophlebitis? What are the alternatives?
No, infusion thrombophlebitis is not grounds for discontinuation of infusions that are essential for the treatment of the case. Thrombophlebitis can be treated by local compressive dressings, NSAIDs (topical and/or systemic)
Case-16
1. What could be the possible factors implicated in elevated glycated HB ( HBA1c ) levels in a previously Non-Diabetic covid patient?














 case-9
case-9








Comments
Post a Comment